Type
Restrictive Mild Malabsorptive
Mechanism of action
Reduce the meal size (Early Satiety)
Mild Reduction of nutrients absorption from the food
Hormonal Effect – Increase GLP1
Expected Weight Loss
70% of excess weight
Brief Description
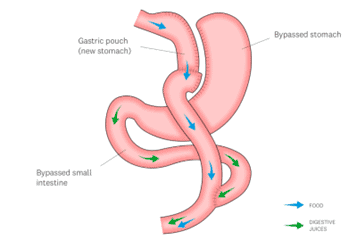
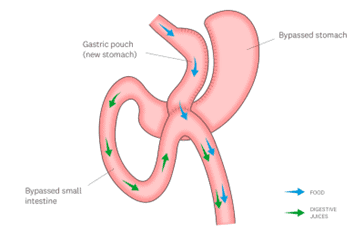
A very small pouch of the upper part of the stomach is created (Separated) using GIA stapler (a device that will cut and seal the edges at the same time), The small bowel is divided at a point 50-60 cm distal to the beginning of it. That will create a proximal and a distal end.
The distal end is joined (Anastomosed) to the small stomach pouch. And the proximal end is rejoined to the small bowel but 1.5 m away from the previous small bowel stomach join.
Doing this will Reduce the meal volume and induce early satiety and make the food passage bypassing the stomach and the first part of the small bowel to reduce the absorption of nutrients from food.